
RANGOON — As scientists continue to learn more about the rise of drug-resistant malaria in Southeast Asia, Burma has become a frontline in the battle to control the disease.
For years, artemisinin-combination therapies (ACTs) have reduced the number of new malaria cases and deaths in the region. But pockets of resistance have emerged, first in Cambodia and also in Burma, with fears that it could continue to spread westward to Africa, where the disease already kills hundreds of thousands of people every year. As a result, experts are discussing whether a rethink in current strategies to combat the parasite is needed.



In Burma, about 70 percent of the population lives in malaria-endemic areas, and the country accounts for most of the malaria-related deaths in the Mekong region. The disease is transmitted through the bites of mosquitos, with the parasite invading the liver and later the red blood cells.
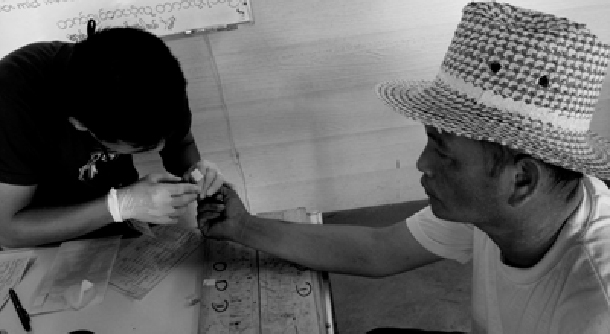
To contain drug resistance, the Ministry of Health’s malaria program has started adopting a strategy in some areas known as DOT, or directly observed therapy, whereby patients are monitored to ensure that they take the full course of their therapy. Stopping medication midway through allows parasites in the body to develop resistance.
But observation can be labor intensive, as the standard treatment regimen for malaria in Burma consists of six separate doses of medication over three days.
DOT is particularly difficult because many of those infected by the disease are migrant workers who are constantly moving, according to Patrick Duigan, the Rangoon-based program manager at the International Organization for Migration.
In the coming years, changing migration patterns will create new challenges, he added. As the economic situation improves in Burma, new transportation routes to neighboring countries will affect the movement of people across borders. The Asean free trade zone planned for 2015 will lead to a further opening of the region, connecting areas of malaria prevalence and drug resistance.
But Burma’s political transition since 2011 has been largely positive for the fight against malaria, particularly in terms of funding. Although the government’s health budget remains minimal, the Global Fund, currently Burma’s biggest contributor to malaria programs, has returned after pulling out of the country under the former regime. It committed US$105 million to malaria programs in Burma from 2011-16, as well as an additional $40 million to the country as part of a regional initiative to eliminate artemisinin resistance.
In a major turn, community-based organizations and ethnic health departments are now being granted permission from the government to work on malaria projects, making them eligible for funding from international donors, said Dr. Adam Richards, a board member and health adviser at the NGO Community Partners International, which provides advice to community-based organizations implementing malaria programs in the country. As a result, these groups can access quality drugs from Rangoon, whereas previously they were forced to transport medication across the border from Thailand.
Different actors are increasingly working together to fight malaria in Burma’s southeast. Last year Thein Sein’s government signed a memorandum of understanding with the Thai government to facilitate cross-border collaboration on public health issues, while private physicians with the Myanmar Medical Association are starting to train government hospital workers in Lower Burma about malaria prevention, diagnosis and treatment.
However, concerns remain about a lack of access to health services in Burma’s Arakan State, especially after the government in February suspended the operations of Medecins Sans Frontieres-Holland (MSF), which provided treatment for more than 10,000 malaria patients.
In order to combat drug resistance, some say it will be necessary to not only contain the parasite, but to eliminate it. This would require significantly more resources, as it would be necessary to ensure that each and every case is caught and treated, including cases where the patients do not show symptoms. It would also be necessary to conduct prevention activities on a much bigger scale.
Burma’s anti-malaria program traces back more than half a century, and in 1963 the country implemented a seven-year elimination plan, but according to Dr. Thaung Hlaing, deputy director of the government’s National Malaria Control Program, elimination was “found to be impossible” due to the inaccessibility of remote areas, poor coverage of mosquito spraying and population movement.
He said the country still lacks the resources to undertake elimination efforts. Instead, the Myanmar Artemisinin Resistance Containment (MARC) program aims to “prevent or at minimum significantly delay the spread of artemisinin-resistant parasites within the country and beyond its borders.”
As part of the program, which began in 2011, the government has tried to ban the sale of oral artemisinin-based monotherapies that contribute to resistance, while promoting combination therapies that use more than a single drug to treat the disease. Efforts are also under way to map the movement of migrant workers, to increase the use of insecticide-treated nets, and to encourage people to spray the insides of their homes with insecticide to kill mosquitos.
“We are a little behind the other Southeast Asian countries because we have been a closed country for decades and we just opened,” Thaung Hlaing told The Irrawaddy. “So while Thailand, Cambodia and Vietnam are trying to do the elimination phase, we can’t at the moment.”
He said pre-elimination activities would likely begin in certain parts of the country between 2015 and 2018 to pave the way for full elimination programs. In the meantime, he said the government had scaled up efforts to control the disease by boosting its annual budget for malaria activities by more than four times, improving supply chain management, increasing community-level diagnosis and treatment, and working with about 20 local and international NGOs as implementing partners.











{kind=link}